


Ebola is terrifying enough in the best possible response conditions.
This is not that.
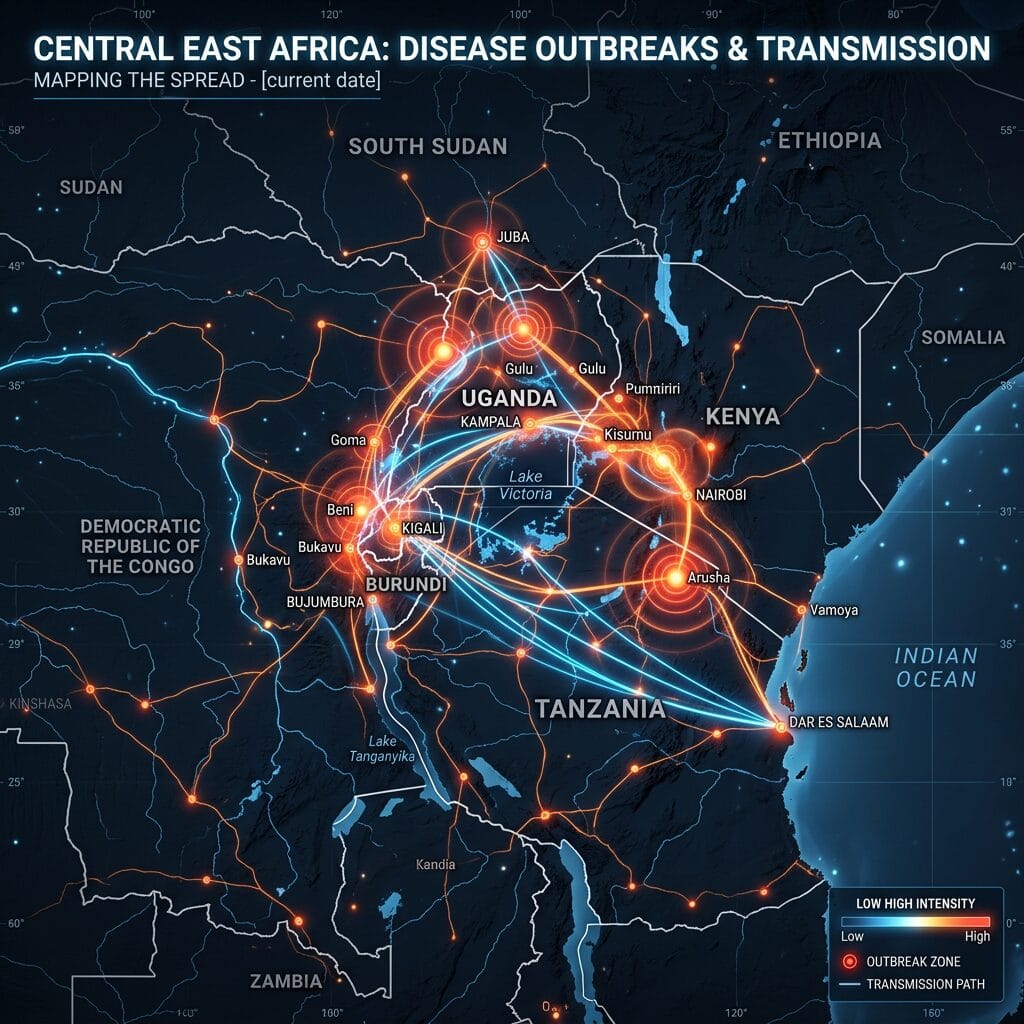
A confirmed Ebola case in South Kivu, far from the outbreak’s known epicentre, shows that Congo’s crisis is spreading across geography, insecurity, and political fragmentation at the same time. The virus is no longer only a public health emergency. It is now moving through one of the hardest environments on earth to manage an outbreak: eastern Congo, where armed groups, distrust, weak surveillance, aid shortages, and contested authority all collide.
That makes this moment especially dangerous.
The Distance From the Epicentre Is the Warning
The confirmed case in South Kivu matters because it appeared hundreds of kilometres from Ituri, where the outbreak was first identified.
That suggests the virus may have been moving quietly before health officials fully understood its reach. Experts already believe the outbreak circulated undetected for around two months before being identified. That kind of delay is deadly with Ebola. Every missed chain of transmission becomes another chance for the virus to travel, spread, and root itself in communities that are not prepared.
This is how outbreaks become harder to contain.
Not all at once, but through invisible movement before the alarm becomes loud enough.
Rebel Control Makes the Response Brutally Complicated
The South Kivu case was reported in territory controlled by a rebel alliance that includes the Rwanda-backed M23 movement.
That changes everything.
Public health responses depend on access, trust, logistics, and clear authority. Rebel-held territory weakens all four. Who controls the roads? Who secures health workers? Who gives permission for contact tracing? Who persuades communities to cooperate? Who guarantees that treatment teams can operate without being attacked, blocked, or politicized?
A virus does not care who controls the territory.
But responders have to care, because insecurity can slow every step.
This Is the Wrong Strain at the Wrong Time
The outbreak involves the Bundibugyo strain of Ebola, a rarer variant with no approved vaccine.
That makes the situation far more dangerous than a response built around a strain with established vaccine tools. Without a ready vaccine, the containment burden falls even more heavily on basic but difficult work: finding cases, isolating patients, tracing contacts, protecting health workers, testing quickly, and ensuring safe burials.
Those steps sound simple from a distance.
In a conflict zone with mistrust and supply shortages, they are anything but simple.
The Numbers Are Already Grim
The reported toll is severe: hundreds of suspected cases, dozens confirmed, and suspected deaths already in the hundreds.
Those numbers are more than statistics. They are evidence of a response racing from behind. They also raise the possibility that the confirmed figures understate the true scale of the crisis. When testing capacity is limited, when communities are suspicious, and when violence disrupts movement, confirmed cases often represent only part of the outbreak.
That is why health experts warning about the “top of the iceberg” should be taken seriously.
With Ebola, what is not yet seen can be as dangerous as what is already counted.
Community Distrust Can Be as Dangerous as the Virus
One of the most alarming developments is the violence around burial practices and treatment sites.
In Ituri, protests reportedly erupted after a family disputed that Ebola caused a death and demanded the body. Tents run by a medical charity were set on fire, and police responded with warning shots and tear gas.
This is not a side issue.
Safe burial is one of the most important tools in Ebola control because bodies remain highly infectious after death. But burial is also deeply emotional and cultural. When families do not trust authorities, when they feel robbed of dignity, or when they believe health workers are lying, containment breaks down fast.
The virus spreads through biology.
The outbreak spreads through mistrust.
Health Workers Are Again Being Asked to Work in Impossible Conditions
Eastern Congo has seen this before.
During the 2018–2020 Ebola outbreak, health centres were attacked repeatedly, and responders had to fight not only the virus but misinformation, fear, and armed violence. Now that pattern threatens to repeat itself. Health workers need protective gear, testing supplies, transportation, security, community support, and enough trust to enter affected areas safely.
Without that, they become targets instead of partners.
And when health workers are threatened, the whole response weakens.
Aid Shortages Are Not an Administrative Problem. They Are a Public Health Risk.
Aid workers say they lack basic supplies, and some link that shortage to foreign aid cuts that weakened local health services and disease surveillance.
That is not bureaucratic background noise. It is central to the story.
Weak surveillance allows outbreaks to circulate undetected. Poor supply chains delay testing and isolation. Underfunded clinics leave health workers exposed. Cuts that look like savings in donor capitals can become death sentences in outbreak zones.
Public health does not fail only when a virus appears.
It fails when the systems meant to catch the virus have already been hollowed out.
Uganda’s Response Shows the Regional Stakes
Two cases have also been confirmed in Uganda, and the country has announced a suspension of flights to Congo as a precaution.
That shows how quickly a national outbreak can become a regional concern. Borders in this part of Africa are not sealed walls. People move for trade, family, work, displacement, and survival. If Ebola spreads across those movements, containment becomes harder and more expensive.
The goal now must be fast regional coordination, not panic.
But pretending this is still only Congo’s problem would be dangerously naïve.
The World Must Move Before This Gets Worse
International funding is starting to arrive, with Britain and the United States announcing support. That matters.
But the response needs more than money. It needs speed, coordination, political access, local trust, security guarantees, testing capacity, and protection for frontline workers. It also needs humility. Communities cannot be treated like obstacles to be managed. They have to be engaged as partners, especially when fear and past trauma shape how people respond to health authorities.
Ebola containment is not only medical.
It is social, political, and logistical.
The Meaning of the Moment
The confirmed case in rebel-held South Kivu is a major warning sign.
It shows the outbreak is not neatly contained near its original epicentre. It shows delayed detection may have allowed wider spread. It shows the virus is entering areas where armed control, community distrust, and aid shortages can cripple the response. And it shows how quickly a rare strain with no approved vaccine can become a regional emergency if containment fails.
Ebola can still be stopped.
But only if the response moves faster than the virus, earns more trust than the rumours, and reaches places where politics and violence have made public health dangerously fragile.

{kind=link}